nUTRITIONAL DISORDERS AND BONE DEFORMITY
A 33 yrs. Lady R. R. came to our Infertility center with 8 wks of gestation with a hope of delivering a healthy baby this time. According to her history, she had 3 spontaneous abortions and two living children, a boy and a girl.
The boy child has a spinal deformity and his MRI of lumbar regions showed extradural lipoma in lower lumbar and sacral spinal canal with multiple congenital defects.
The baby girl also has scoliosis.
A detailed investigation of the present conception was carried out including Total Blood Count, Random Blood glucose, Routine Urinanalysis, Alpha fetoprotein were normal while TORCH IgG was positive. Under our antenatal care Dydrogesterone was given as luteal support till complete placentation. As anti-TORCH Spiromycin 3mIU daily was provided along with Folic acid and Vitamin tablets till 20 weeks. Later Iron & Calcium were added till delivery. Isoxuprine was provided as emergency treatment for any pain in the abdomen. As prophylaxis part of antenatal care, Tetanus Toxoid injections were given at 21 & 24 weeks.
A healthy baby boy was delivered by Caesarean section. The baby was specially investigated for any bone deformities, no abnormalities were detected. Now the boy is 3.5 years old.
After one year her younger sister Lady R. A. 27 yrs. came for similar treatment. She has a history of 1 spontaneous abortion at 3 .5 months of gestational age.She was provided hormone supplement according to her hormone levels. After 5 months she came to infertility centre with 7 weeks gestation.
She has a baby girl of 4 yrs.with kyphotic bone deformity.
Similar routine investigations were done. She did not have TORCH infection. Thus everything else Blood Count, Random Blood glucose, Routine Urinanalysis & Alpha fetoprotein tested & were found normal. Dydrogesterone was given as luteal support till complete placentation. Folic acid and Vitamin tablets were added from the first trimester, later Iron & Calcium were added till delivery. Isoxuprine was provided as emergency treatment for any pain in the abdomen. As prophylaxis part of antenatal care, Tetanus Toxoid injections were given at 21 & 24 weeks.
The younger sister also had a normal delivery with a healthy baby boy who also does not have any bone or joint deformities. Now the boy is 2 years old.
Both the sisters are happy but they have preserved cord blood for any future use.






 Counselling Infertility
Counselling Infertility Our team
Our team 22 years of Service (Since 1992)
22 years of Service (Since 1992) In Vitro Fertilization
In Vitro Fertilization Celebrating 20 years of Service
Celebrating 20 years of Service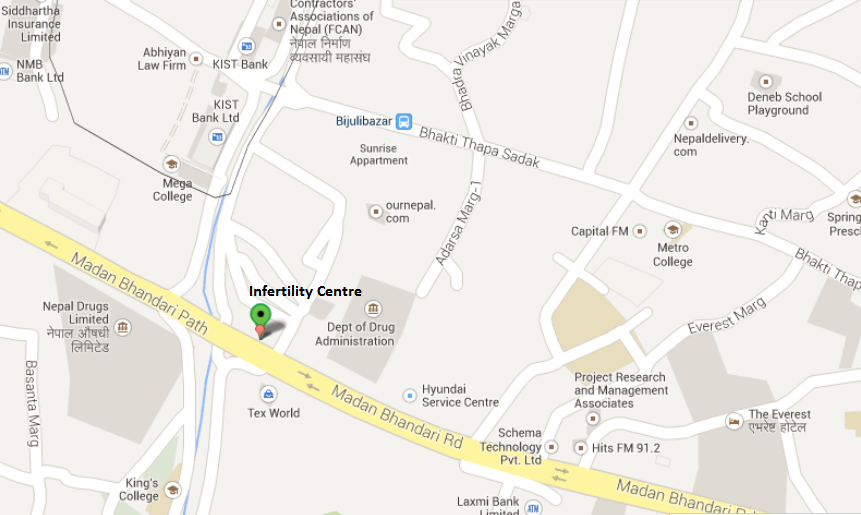







{kind=link}